{kind=link}

421 items | 373 visits

Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease.
Siri-Tarino PW, Sun Q, Hu FB, Krauss RM.
Am J Clin Nutr. 2010 Jan 13. [Epub ahead of print]
PMID: 20071648
doi:10.3945/ajcn.2009.27725
Conclusions: A meta-analysis of prospective epidemiologic studies showed that there is no significant evidence for concluding that dietary saturated fat is associated with an increased risk of CHD or CVD. More data are needed to elucidate whether CVD risks are likely to be influenced by the specific nutrients used to replace saturated fat
"Scientists have proved for the first time that fructose, a cheap form of sugar used in thousands of food products and soft drinks, can damage human metabolism and is fueling the obesity crisis.
Fructose, a sweetener usually derived from corn, can cause dangerous growths of fat cells around vital organs and is able to trigger the early stages of diabetes and heart disease.
Over 10 weeks, 16 volunteers on a controlled diet including high levels of fructose produced new fat cells around their heart, liver and other digestive organs. They also showed signs of food-processing abnormalities linked to diabetes and heart disease. Another group of volunteers on the same diet, but with glucose sugar replacing fructose, did not have these problems."
Vitamin D, nervous system and aging.
P. Tuohimaa, T. Keisala, A. Minasyan, J. Cachat and A. Kalueff. .
Psychoneuroendocrinology, Volume 34, Supplement 1, December 2009, Pages S278-S286
NEUROACTIVE STEROIDS: EFFECTS AND MECHANISMS OF ACTION
doi:10.1016/j.psyneuen.2009.07.003
This is a mini-review of vitamin D3, its active metabolites and their functioning in the central nervous system (CNS), especially in relation to nervous system pathologies and aging. The vitamin D3 endocrine system consists of 3 active calcipherol hormones: calcidiol (25OHD3), 1α-calcitriol (1α,25(OH)2D3) and 24-calcitriol (24,25(OH)2D3). The impact of the calcipherol hormone system on aging, health and disease is discussed. Low serum calcidiol concentrations are associated with an increased risk of several chronic diseases including osteoporosis, cancer, diabetes, autoimmune disorders, hypertension, atherosclerosis and muscle weakness all of which can be considered aging-related diseases. The relationship of many of these diseases and aging-related changes in physiology show a U-shaped response curve to serum calcidiol concentrations. Clinical data suggest that vitamin D3 insufficiency is associated with an increased risk of several CNS diseases, including multiple sclerosis, Alzheimer's and Parkinson's disease, seasonal affective disorder and schizophrenia. In line with this, recent animal and human studies suggest that vitamin D insufficiency is associated with abnormal development and functioning of the CNS. Overall, imbalances in the calcipherol system appear to cause abnormal function, including premature aging, of the CNS.
"For what reason I don't know, but this January 2009 editorial by William Faloon of the Life Extension Foundation is making the rounds. Perhaps it just came available on the web.
It's a good read, particularly in light of the billions and trillions of dollars the thieves & thugs in DC are about to flush down the crapper on your behalf. Some notable excerpts.
A large number of new vitamin D studies have appeared in the scientific literature since I wrote my plea to the federal government. These studies don’t just confirm what we knew 16 months ago—they show that optimizing vitamin D intake will save even more lives than what we projected.
For instance, a study published in June 2008 showed that men with low vitamin D levels suffer 2.42 times more heart attacks. Now look what this means in actual body counts.
Each year, about 157,000 Americans die from coronary artery disease-related heart attacks. Based on this most recent study, if every American optimized their vitamin D status, the number of deaths prevented from this kind of heart attack would be 92,500.
To put the number of lives saved in context, tens of millions of dollars are being spent to advertise that Lipitor® reduces heart attacks by 37%. This is certainly a decent number, but not when compared with how many lives could be saved by vitamin D. According to the latest study, men with the higher vitamin D levels had a 142% reduction in heart attacks."
Genetic variants associated with Lp(a) lipoprotein level and coronary disease.
Clarke R, Peden JF, Hopewell JC, Kyriakou T, Goel A, Heath SC, Parish S, Barlera S, Franzosi MG, Rust S, Bennett D, Silveira A, Malarstig A, Green FR, Lathrop M, Gigante B, Leander K, de Faire U, Seedorf U, Hamsten A, Collins R, Watkins H, Farrall M; PROCARDIS Consortium.
N Engl J Med. 2009 Dec 24;361(26):2518-28.
PMID: 20032323
Conclusions We identified two LPA variants that were strongly associated with both an increased level of Lp(a) lipoprotein and an increased risk of coronary disease. Our findings provide support for a causal role of Lp(a) lipoprotein in coronary disease.
"23/12/2009
Convincing evidence that a third type of cholesterol plays a role in causing heart disease
Prof WatkinsNew BHF-funded research from the University of Oxford shows that a type of cholesterol called Lipoprotein(a) definitely plays a role in causing heart disease.
Published today in the New England Journal of Medicine, the findings could add new medicines to doctors' toolkits for preventing heart disease, and open new avenues of research for treatments.
Lipoprotein(a), or Lp(a), has been associated with heart disease since the 1990s, but until now it has not been possible to distinguish whether it actually causes heart disease. Now a study analysing the genes of nearly 16,000 people from the UK and across Europe has provided evidence that two variations of the gene for Lp(a) are strongly linked to heart disease risk, indicating a causal role in disease development."
"Strongest evidence yet that Lp(a) causes heart disease
December 23, 2009 | Lisa Nainggolan
Oxford, UK - New genetic research has identified two relatively rare single nucleotide polymorphisms (SNPs) that explain just over a third of the variance in lipoprotein(a) (Lp[a]) levels in individuals of European descent [1]. The work confirms unequivocally that Lp(a) is a causal factor for coronary disease, say Dr Robert Clarke (University of Oxford, UK) and colleagues in their paper in the December 24, 2009 issue of the New England Journal of Medicine.
"This is the most convincing evidence so far that this protein [Lp(a)] is directly part of the pathway that causes heart disease rather than a bystander. If we can target it through treatment, we might expect to lower the risk of disease," coauthor Dr Hugh Watkins (University of Oxford) told heartwire. "
"These are the slides from the within-countries discussion on cholesterol and heart disease. I've allowed the sarcasm back in, which was strictly limited when the slides were originally presented. OK, there is a correlation. In fact, if you are a bloke, having a cholesterol above that certain magic number on the graph is clearly catastrophic and boy, are you in trouble. No statins to save your life in those days!"
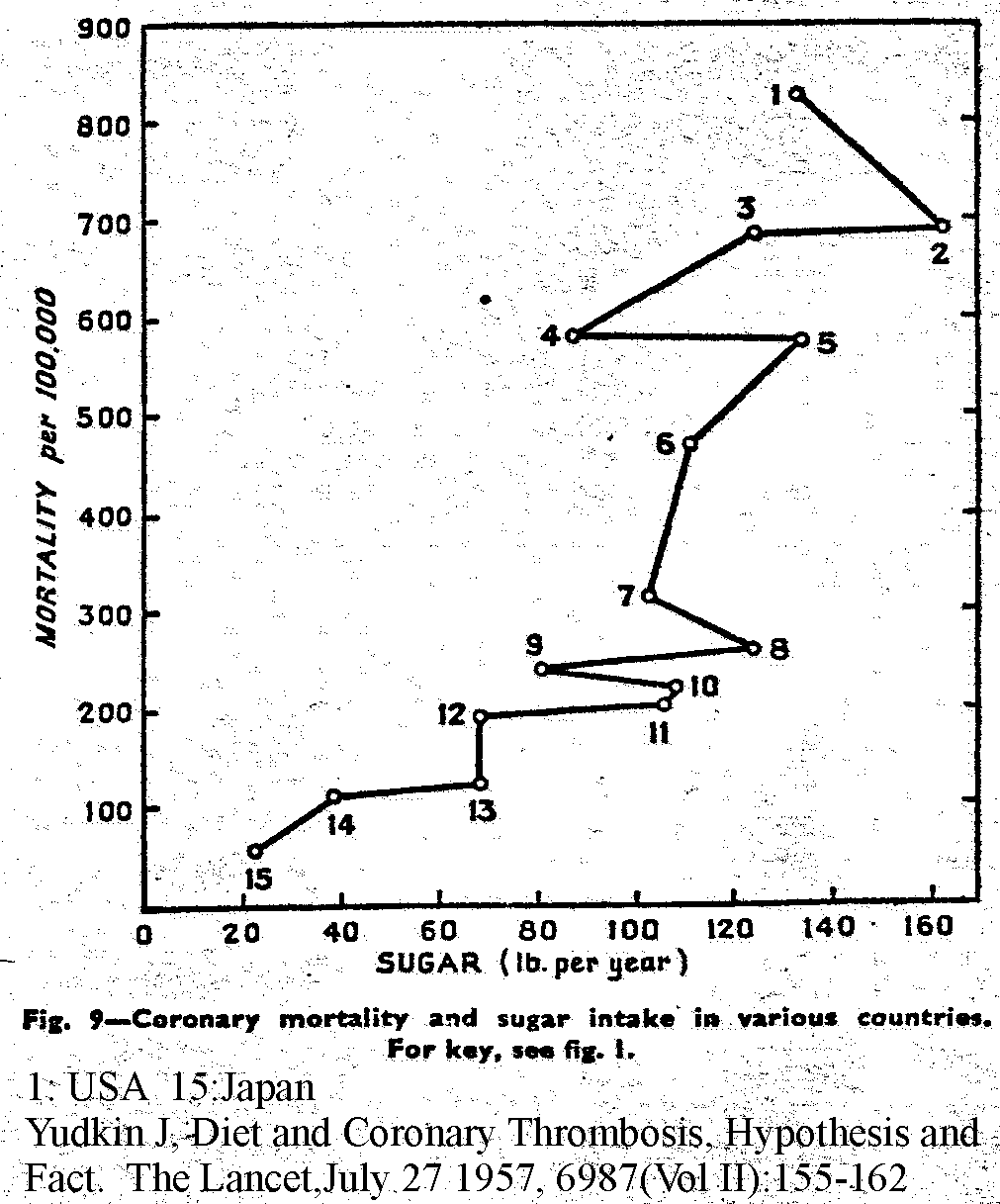
Diet and Coronary Thrombosis., Hypothesis and Fact
Yudkin J.
The Lancet 1957.
(Figure 9 only)
"What Are Nutritional Diseases?
In their book, The Modern Nutritional Diseases, Fred and Alice Ottoboni, retired Public Health Service scientists, list the following.
• Obesity
• Diabetes II
• Cardiovascular Diseases
• Stroke.
• Cancer.
Modern nutritional diseases are just that. They haven't always been the ugly part of our life. They were introduced when people had to get their food from grocery stores, when people traded their whole foods from the family farm for those manufactured by the food processing industry. "
"Coronary Heart Disease Mortality and Blood Cholesterol
In the Seven Countries study, there were great differences in coronary heart disease (CHD) mortality at similar blood cholesterol levels.
In this study Dr. Keys pointed to a correlation between deaths from coronary heart disease and serum cholesterol in 15 populations in seven countries.
Dr Ravnskov plotted his original data which was not available in the research summaries. Particularly interesting were differences between two localities within the same country or nearby islands in each of 4 of the seven countries.
West Finland had about 45 CHD (coronary heart disease) deaths at a median cholesterol level of 250 mg/dl. However North Karelia, also in Finland, had over 200 CHD deaths at about 260 mg/dl.
The island of Crete had only 20 CHD deaths at cholesterol levels of about 200. The nearby island of Corfu had about 85 CHD deaths at a cholesterol level of about 190 mg/dl."
"Here's a page or so (p163-4) from John Yudkin's book "Pure White and Deadly", 1972 edition. Yudkin begins the chapter with an apology for talking about such uncomfortable disagreements in public. But he liked the truth.
This quote covers opinion from Prof John Yudkin and Dr Meyer Friedman. You can hear their dislike of Keys. Keys was the architect of what has become the current world obesity epidemic and never one to let the truth get in the way of a good idea, as with his six nations "fat causes heart disease" study. Unfortunately Meyer's list of those easily misled did not include gullible politicians who set food policy. Keys was a very successful politico, with intense conviction of his own correctness. Fine if he had been right, which he wasn't."
Calcium:magnesium ratio in local groundwater and incidence of acute myocardial infarction among males in rural Finland.
Kousa A, Havulinna AS, Moltchanova E, Taskinen O, Nikkarinen M, Eriksson J, Karvonen M.
Environ Health Perspect. 2006 May;114(5):730-4.
doi:10.1289/ehp.8438
PMID: 16675428
Results of this study with specific Bayesian statistical analysis support earlier findings of a protective role of Mg and low Ca:Mg ratio against coronary heart disease but do not support the earlier hypothesis of a protective role of Ca
Overview and perspective in human nutrition.
Willett WC.
Asia Pac J Clin Nutr. 2008;17 Suppl 1:1-4. Review.
PMID: 18296289
For the last decade, the focus of nutritional advice for prevention of chronic disease has been to limit or reduce
total fat intake and to consume large amounts of carbohydrate. However, this advice is inconsistent with many
lines of evidence indicating that unsaturated fats have beneficial metabolic effects and reduce risk of coronary
heart disease. More recent evidence has also shown that the large majority of carbohydrates in Western diets,
consisting of refined starches and sugars, have adverse metabolic effects and increase risks of coronary heart
disease and type 2 diabetes. Unfortunately, a major opportunity for health improvement has been lost by failing
to distinguish healthy from unhealthy forms of carbohydrates and fats. Recent analyses indicate that moderate
changes in diet, together with regular physical activity and not smoking, can prevent the large majority of heart
disease, type 2 diabetes, and some forms of cancer. These findings have substantial relevance for many populations
in Asia, where incidence of type 2 diabetes is rising rapidly.
"Wednesday, May 27, 2009
Eicosanoids and Ischemic Heart Disease, Part II
Here's where it gets more complicated and more interesting. The ratio of omega-6 to omega-3 matters, but so does the total amount of each. This is a graph from a 1992 paper by Dr. Lands:
In sum, this suggests that the single best way to avoid a heart attack is to reduce omega-6 consumption and ensure an adequate source of omega-3. The lower the omega-6, the less the omega-3 matters. This is a nice theory, but where's the direct evidence? In the next post, I'll discuss the controlled trial that proved this concept once and for all: the Lyon diet-heart trial.
Reducing the Burden of Disease Through Adequate Intake of Vitamin D3.
A presentation at University of California, San Diego,
April 9, 2008
by William B. Grant, Ph.D
"Ann Arbor, MI - New laboratory research suggests that the COX-2 inhibitor celecoxib (Celebrex, Pfizer), might impede the action of "baby" aspirin [1]. Dr Gilad Rimon (University of Michigan, Ann Arbor) and colleagues found evidence that this was the case in a dog model and say that "it will be important to determine" whether the same is true in humans.
The report was published online December 1, 2009 in the Proceedings of the National Academy of Medicine.
Celecoxib is the only COX-2 inhibitor to have remained on the market in the US, and doctors who recommend this painkiller often coprescribe a daily low dose of 81 mg of aspirin (known as a "baby" dose) to counteract any possible prothrombotic effects of the coxib, while minimizing potential gastrointestinal toxicity of the aspirin.
Senior author of the new work, Dr William L Smith (University of Michigan, Ann Arbor), explained to heartwire that previous studies in humans have shown that celecoxib does not interfere with the effect of a standard dose of aspirin (325 mg), but any potential interaction of celecoxib with the lower dose has not been examined.
Stagger dosing to avoid any potential problems
First, Smith explained that he and his colleagues looked in vitro at celecoxib and found that it binds to one of two available sites on the COX-1 enzyme. "This surprised us," he commented. "It appears to interfere with the ability of some other drugs to affect COX-1, most notably aspirin."
Second, in beagles, they administered the dog-equivalent of a baby dose of aspirin in humans and then gave some of the animals the equivalent of 100 mg of celecoxib twice daily in addition. "Celecoxib plus aspirin interfered with the normal effect of low-dose aspirin on platelets," he notes.
Smith says this observation obviously requires confirmation in humans, but in the meantime he suggests "getting around the problem" by patients taking the low-dose aspirin at least 15 to 30 minutes before the celecoxib is taken, "because the effect of aspirin on platelets is rather qui
C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis.
The Lancet, Early Online Publication, 22 December 2009
doi:10.1016/S0140-6736(09)61717-7
Interpretation
CRP concentration has continuous associations with the risk of coronary heart disease, ischaemic stroke, vascular mortality, and death from several cancers and lung disease that are each of broadly similar size. The relevance of CRP to such a range of disorders is unclear. Associations with ischaemic vascular disease depend considerably on conventional risk factors and other markers of inflammation.
"Largest-ever meta-analysis finds CRP is unlikely to be causal for CVD
December 21, 2009 | Lisa Nainggolan
Cambridge, UK - In the largest and most comprehensive meta-analysis to date looking at C-reactive-protein (CRP) levels and risk of coronary heart disease (CHD) and stroke, British researchers conclude that CRP is unlikely to be a causal factor for cardiovascular disease [1].
Although CRP concentration was linearly associated with CHD, stroke, and vascular mortality, as well as nonvascular mortality, statistical adjustment for conventional cardiovascular risk factors "resulted in considerable weakening of associations," note the scientists of the Cambridge-based Emerging Risk Factors Collaboration (ERFC), who report their findings online December 21, 2009 in the Lancet.
In an editorial accompanying the paper [2], Drs S Matthijs Boekholdt and John JP Kastelein (Academic Medical Center, Amsterdam, the Netherlands) say the UK authors "are to be commended for this impressive data set." Although the findings "add weight to the evidence of noncausality" for a role of CRP in the development of cardiovascular disease, "the debate can be resolved only by randomized trials with agents that specifically target CRP, and such compounds are currently under development," say the Dutch doctors.
Commenting on the new meta-analysis for heartwire, Dr Paul Ridker (Brigham and Women's Hospital, Boston, MA), a long-time advocate of CRP and the lead investigator of the JUPITER trial, said: "Whether or not CRP is 'causal' for heart disease is neither the crucial issue at hand nor relevant for public health. What is crucial is getting international agreement that CRP identifies higher-risk individuals who would not otherwise qualify for a life-saving therapy, and then showing that such individuals clearly benefit from treatment. The new meta-analysis demonstrates the former, and JUPITER demonstrates the latter." "
Endothelial-Vasoprotective Effects of High-Density Lipoprotein Are Impaired in Patients With Type 2 Diabetes Mellitus but Are Improved After Extended-Release Niacin Therapy.
Sorrentino SA, Besler C, Rohrer L, Meyer M, Heinrich K, Bahlmann FH, Mueller M, Horváth T, Doerries C, Heinemann M, Flemmer S, Markowski A, Manes C, Bahr MJ, Haller H, von Eckardstein A, Drexler H, Landmesser U.
Circulation. 2009 Dec 21. [Epub ahead of print]
PMID: 20026785
doi: 10.1161/CIRCULATIONAHA.108.836346
Conclusions—HDL from patients with type 2 diabetes mellitus and metabolic syndrome has substantially impaired endothelial-protective effects compared with HDL from healthy subjects. ER niacin therapy not only increases HDL plasma levels but markedly improves endothelial-protective functions of HDL in these patients, which is potentially more important
421 items | 373 visits